This article continues our series of white papers on radiologic patient positioning techniques that appear each month on AuntMinnie.com. The series will explore each of the major modalities. If you’d like to comment on or contribute to this series, please e-mail [email protected] .
Chest x-ray AP positioning techniques
Anteroposterior (AP) chest radiographs can be made in the intensive care unit, the operating suite, or the patient’s room using mobile equipment. They are often known as a portable film when performed with a mobile unit. They are generally of lesser quality than a posteroanterior (PA) radiograph or recumbent films made in the radiology department. Hence, it is preferable to obtain a film in the radiology department unless the patient cannot be moved without hazard.
Ask the patient to remove clothes from the waist up, put on a hospital gown, remove any jewelry (necklace, earrings), and, if necessary, tie hair up on top of the head.
Patient position considerations
Instruct the patient to lie supine or upright, with the back against the grid. If the patient’s condition allows, raise the head end of the cart, as the semi-erect position will improve the anatomical details.
Positioning is difficult in a hospital bed, thus the patient’s true position is often unknown, which causes difficulty in assessing pulmonary vascularity or the presence of pleural fluid. If a portable film must be done, an upright portable film is preferable to a supine film. The patient’s position and the distance from the x-ray tube to the film should be recorded on the film cassette.
Position of chest
Film holder placement
For AP chest radiographs, the recommendation is to place the cassette film holder or image receptor (IR) crosswise, not lengthwise, using a 14 x 17-inch (35 x 43-cm) IR. Place the IR behind or underneath the patient. The lengthwise use of the IR can cut off the side borders of the lung fields. The cassette should be adjusted so that the upper border is approximately 1 1/2 to 2 inches (3.8-5 cm) above the shoulders.
The central ray (CR) is set perpendicular to the long axis of the sternum and the center of the cassette. The jugular notch is the recommended landmark for the location of the CR for AP chest radiographs. The notch is used for locating the center of the lung fields at the T7 level (mid-thorax).

The T7 level on an average adult is 3-4 inches (8-10 cm) below the jugular notch. For older or thinly built patients it is 3 inches (8 cm) below the jugular notch, and for patients with athletic physiques it can be as much as 5 inches. This distance can be estimated by using your hand. The average-size hand, with fingers together, is approximately 3 inches. In patients with kyphosis, a slight cephalad angulation may be needed.
The upper border of the illuminated field should be above the shoulders and on each side. It should correspond to the outer skin margins.
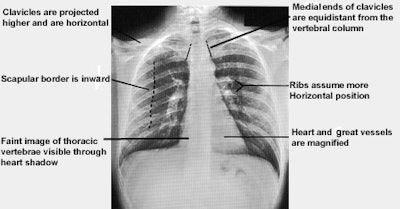
Evaluation criteria for a good AP projection
Chest x-ray lateral projection positioning techniques
A lateral chest projection is part of standard x-ray examination of the chest. Although the PA view is the mainstay of diagnosis, it provides a clear view of only about 80% of the lungs; the retrosternal and retrocardiac spaces as well as the posterior sulci are obscured by overlying anatomy. The lateral view clearly displays these areas and is especially useful in detecting lower-lobe lung disease, pleural effusions, and anterior mediastinal masses.
Ask the patient to remove clothes from the waist up, put on a hospital gown, remove any jewelry (necklace, earrings), and, if necessary, tie hair up on top of the head.

Adjust the patient so that the left shoulder is firmly against the film cassette, and the lower-left chest wall is no more than 1-2 inches away from the cassette. The goal is to have the midsagittal plane of the body vertical and parallel with the cassette.

For a lateral projection, the chest landmark used for locating the center of the lung fields is at the T7 level (mid-thorax). The T7 level on an average adult is 3-4 inches (8-10 cm) below the jugular notch. For patients with an athletic physique, T7 can be as much as 5 inches below the jugular notch. The chest landmark corresponds to the inferior angle of the scapula. The CR should be positioned perpendicular and midline to the film cassette.
Film holder placement
Place the film cassette holder (or IR) crosswise or lengthwise depending on the patient’s physique, using a 14 x 17-inch (35 x 43-cm) IR. Place the IR against the left side of the patient. Adjust the height of the cassette so the upper border is 1 1/2 to 2-inches above the shoulder.
The upper border of the illuminated field should be above the shoulders and on each side. It should correspond to the outer skin margins.
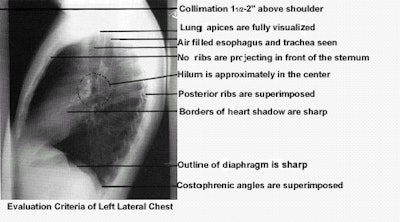
Evaluation criteria for a good lateral chest projection